Mosaic Life Care is a regional hospital based out of St. Joseph, MO that is 50 miles from Kansas City, MO. Although it is a community hospital, it has an excellent interventional pulmonology practice that uses cutting-edge robotic navigation bronchoscopy systems to provide the best care for its patients.
Before the implementation of the ROSE Prep™ system, Mosaic Life Care’s interventional pulmonology practice faced significant challenges in its bronchoscopy procedures. Some of their challenges include (1) significant time taken to get the confirmation that adequate cells are present for diagnosis, (2) uncertainty in knowing whether enough diagnostic cells are present for molecular analysis, and (3) an increase in the overall procedure time.
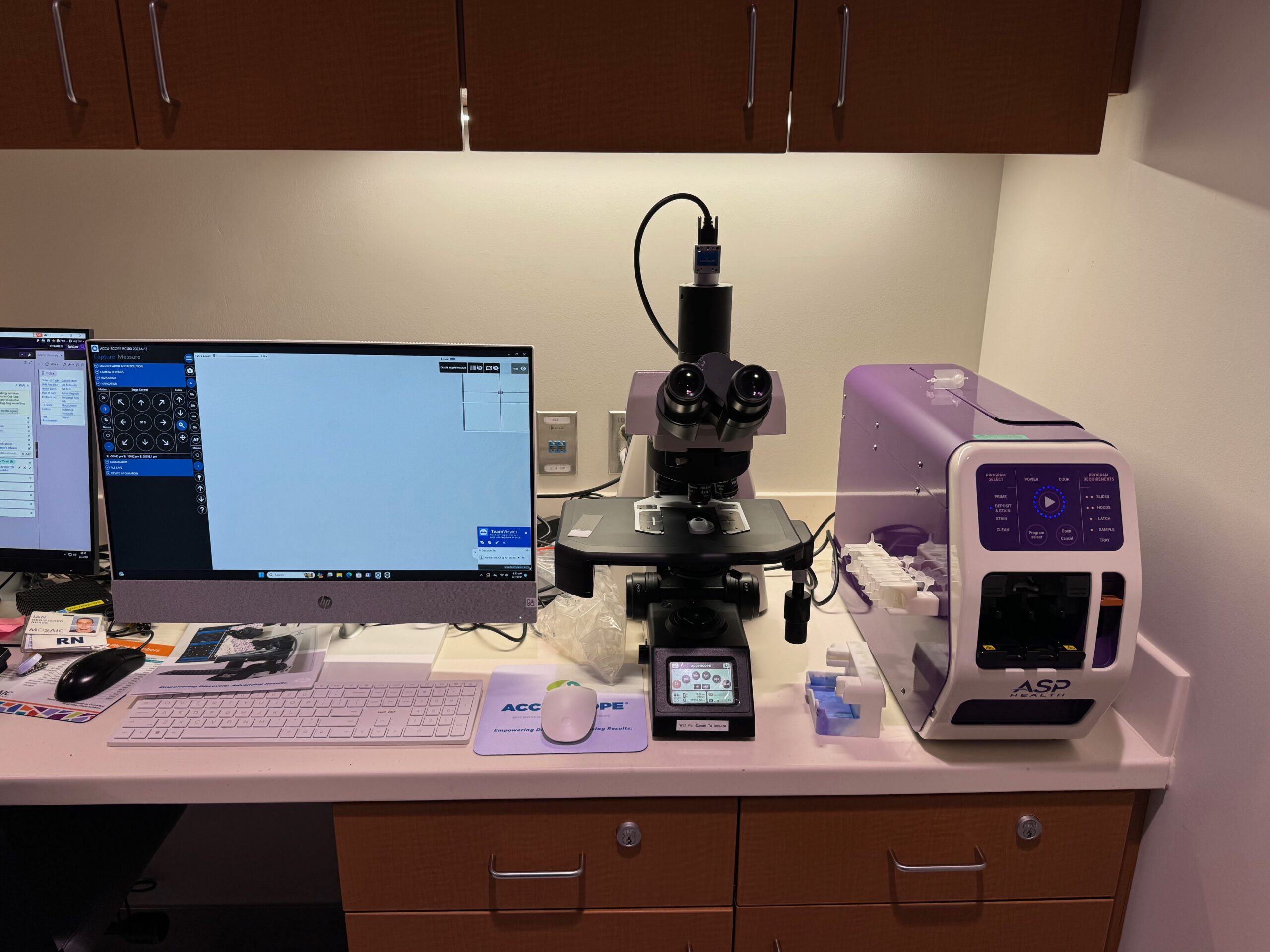
ASP Health in collaboration with Dr. Gautam Balakrishnan, Interventional Pulmonologist at Mosaic Life Care, and his team implemented a fully automated Rapid On-site Evaluation solution. This involved setting up both ASP Health’s ROSE Prep™ system and Accuscope’s RC-500 Remote Microscope solution within the bronchoscopy suite. (ASP Health and Accuscope have a non-exclusive relationship to cross-sell their products to their customers).
The pulmonary nurses at Mosaic Life Care underwent a quick 30-minute training on the ways to use both the ROSE Prep pro system and Accuscope’s RC-500. The overall procedure workflow was as follows:
- After the fine needle aspirate sample was obtained by the interventional pulmonologist as part of the bronchoscopy procedure, the entire sample was loaded into ASP’s proprietary Sample Vial by a pulmonary technician.
- The ASP Vial™ was then passed onto a pulmonary nurse who thoroughly homogenized the sample with a small amount of buffer by simply massaging the easy-to-use sample vial.
- Two drops of the fully homogenized sample were then loaded into ASP’s unique sample pod, which was then inserted into the ROSE Prep™ system.
- The other consumables such as the glass slides and sample hoods were inserted into the ROSE Prep pro system before initiating the automated sample preparation and staining of the FNA sample.
- The remaining needle aspirate sample in the ASP™ Vial was then transferred to a formalin jar for downstream cell block preparation.
- The automatically prepared specimen slide (specimen preparation time including staining is ~ 100 seconds) was then manually removed from the ROSE Prep™ system by the pulmonary nurse and then loaded onto Accuscope’s RC-500 remote microscope system.
- Once the fully prepared specimen slide was loaded onto the RC-500 system, the cytotechnologist who was present at a remote location quickly assessed the slide and provided the adequacy assessment of the diagnostic cells present on the specimen slide to the interventional pulmonologist over the phone.
In summary, at Mosaic Life Care, the entire Rapid On-site Evaluation was implemented without the need for the cytotechnologist or the cytopathologist to be present in the bronchoscopy suite.
The main advantage of the RC-500 system is that it can be remotely operated making it easy for the cytopathologists and cytotechnologists to perform Rapid On-site Evaluation without having to be present directly in the bronchoscopy suite. While this fully automated and remote ROSE implementation led to a slight increase in the work of the pulmonary nurses, the ones at Mosaic Life Care preferred this solution compared to having to work several flights of stairs to go between the bronchoscopy suite and the pathology lab.
The interventional pulmonologist at Mosaic Life Care was also excited as it reduced the overall time from obtaining the FNA to getting the adequacy feedback to less than 5 minutes compared to approximately 15 minutes when following their previous workflow.
ASP Health believes that this partnership and the implementation of the ROSE PrepTM pro system in combination with a remote microscope system can democratize the Rapid On-site Evaluation practice wherein the smaller regional and community hospitals can provide the best in care service to its patients which were once reserved for large academic medical centers and large pulmonary practices.
